
“Does Seroxat have a capacity to cause asverse effects consequent upon or following discontinuance (withdrawl) such as prevent or make more difficult the ability of users to discontinue, withdraw from or remain free from taking Seroxat to a greater extent than all other Selective Serotonin Re-uptake Inhibitors (SSRIs)”
........... NB - spelling errors as per original document.
HM Courts Service: Seroxat Group Litigation Order no: 68.specifying that the adverse effects of Seroxat are or have to be proven to be
“greater extent than all other Selective Serotonin Re-uptake Inhibitors (SSRIs)”it appears the deciding factor of the Seroxat litigation – given venlafaxines’ shortest 5 hour half life– is dependant on each drugs classification.
In the “Halting SSRIs” document Dr David Healy opines (excerpt below) that venlafaxine is an SSRI up to doses of 150 mg.

{kind=link}
The work by the Committee on Safety of Medicines (CSM), Expert Working Group (EWG) on SSRI Antidepressants, who’s report was published December 2004 confirms this aspect
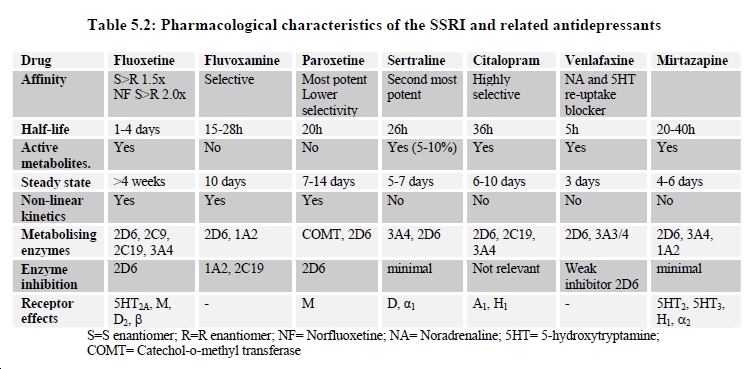
“……When compared with tricyclic antidepressants, they are certainly more selective but still affect neurotransmitters other than serotonin in the central nervous system 8. This can be illustrated with reference to their binding affinities to the different monoamine transporters (table 5.1) 9. Furthermore, their effect is not limited to uptake inhibition. They have primary effects on many different receptors (see table 5.2), and also cause secondary changes in receptor numbers and receptor function at the synapse 8 10 11. The same principles also apply to the related antidepressants venlafaxine (which is mixed serotonin and noradrenaline reuptake inhibitor) and mirtazapine (which acts as an antagonist at the α2, 5HT2, 5HT3 and H1 receptors).”The CSM EWG report Table 5.2 (below) shows the “Affinity” of each drug included in their investigation with reference to the “selective” nature and potency.

{kind=link}
………NB – The CSM Report was carried out prior to the SNRI duloxetine (Eli Lilly, Yentreve, Cymbalta – part developed by Boehringer Ingelheim) being licensed.
The findings show
citalopram (Lundbeck, Cipramil, Celexa) -- was - “highly selective”
sertraline (Pfizer, Lustral Zoloft) -- was the - “Second most potent”
paroxetine (GSK, Seroxat Paxil) -- was the - “Most potent, Lowest selectivity”
venlafaxine (Wyeth, Efexor Effexor) -- is listed as a - “re-uptake blocker” of NA = Noradrenaline and 5HT = 5-hydroxytryptamine = Serotonin
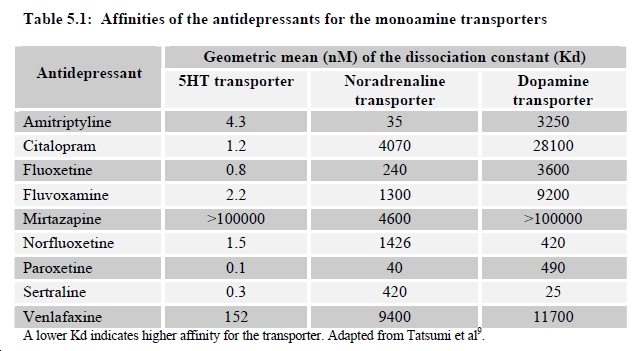
The CSM EWG report Table 5.1 (below) adapted from Tatsumi et al “Pharmacological profile of neuroleptics at human monoamine transporters” study paper originally published in the European Journal of Pharmacology 1999;368(2-3):277-83 shows the “Affinity” of each drug included in their investigation with reference to the potency of effects on three monoamine transporters, 5HT = serotonin, NA = noradrenaline and DA = dopamine.

{kind=link}
………NB – The CSM Report was carried out prior to the SNRI duloxetine (Eli Lilly, Yentreve, Cymbalta – part developed by Boehringer Ingelheim) being licensed.
The findings are valued using Kd or dissociated constant – as explained on the table the lower the Kd the higher the affinity to the transporter. Ignoring the tricyclic antidepressant comparator Amitriptyline and Norfluoxetine the drug Seproxetine which was investigated by Eli Lilly as an antidepressant, development was never completed and the drug as yet not marketed.
The findings -- Affinity Kd and (potency rating) -- show
citalopram - 1.2 Serotonin (Fourth) – 4070 Noradrenaline (Fifth) – 28100 Dopamine (Sixth)
sertaline - 0.3 serotonin (Second) – 420 noradrenaline (Third) - 25 Dopamine (First)
paroxetine - 0.1 serotonin (First) – 40 noradrenaline (First) - 490 Dopamine (Second)
venlafaxine - 152 serotonin (Sixth) – 9400 noradrenaline (Seventh) – 11700 Dopamine (Fifth)
In terms of classification and license applications it appears that Wyeth (now part of Pfizer) and Eli Lilly with their drugs venlafaxine, (Efexor Effexor) and duloxetine, (Yentreve, Cymbalta) are the only manufacturers to have been open in declaring the drugs additional action on noradrenaline (NA), in the case of Wyeth’s venlafaxine noradrenaline (NA) and dopamine (DA).
Venlafaxine is the only drug included in the CSM EWG investigation classified as an SNRI - however, according to the Tatsumi et al study accepted by the CSM EWG of the drugs classified as SSRIs – five have a higher Affinity and Potency to serotonin (5HT) – but six have a higher Affinity and Potency to noradrenalin (NA) - and four a higher Affinity and Potency to dopamine (DA).
Both SSRIs, Sertraline (Lustral, Zoloft) and paroxetine (Seroxat, Paxil), have considerably higher Affinity and Potency to all three transporters than the SNRI venlafaxine (Efexor, Effexor).
The SSRI Sertraline (Lustral, Zoloft) has at, Kd 0.3 the second highest Affinity and Potency to serotonin (5HT) and at Kd of 25 the highest Affinity and Potency to dopamine (DA), higher than all other drugs in the class.
The SSRI paroxetine (Seroxat, Paxil), at Kd 0.1 has the highest Affinity and Potency to Serotonin (5HT) and is the highest in Affinity and Potency, at Kd 40, to noradrenaline (NA) higher than all other drugs in the class.
The word “selective” seems to be an ambiguous descriptor of little or no value - all drugs in the SSRI, SNRI class, because they are not “pharmacologically “clean””, appear to have clear and unmistakable claim to being Serotonin, Noradrenaline and Dopamine Re-uptake Inhibitors.
With regard the SSRI v SNRI Issue – it appears the question is not whether venlafaxine can be considered an SSRI – but possibly whether paroxetine is actually an SNRI?
No comments:
Post a Comment