
“Does Seroxat have a capacity to cause asverse effects consequent upon or following discontinuance (withdrawl) such as prevent or make more difficult the ability of users to discontinue, withdraw from or remain free from taking Seroxat to a greater extent than all other Selective Serotonin Re-uptake Inhibitors (SSRIs)”HM Courts Service: Seroxat Group Litigation Order no: 68.
……….. NB - spelling errors as per original document.
appears to be solely based on Seroxats’ discontinuation problem being worse “than all other” SSRIs raises several questions with regard the propagation, collection, presentation and analysis of adverse drug reaction (ADR) reports; and the Medicines and Healthcare products Regulatory Agency (MHRA) the executive agency of the UK Governments Department of Health responsible for interpretation of the Yellow Card Scheme generated statistical drug analysis data and their ethics in accepting media (BBC Panorama) generated Yellow Card documentation - some collected through the Seroxat User Group.org website and support group, set up by Solicitor Hugh James for litigants.
It also raises the question of what the experts consider the cause of the discontinuation problem to be in relation to the pharmacokinetics of each drug in the class and which drugs are included in the SSRI class.
The “Halting SSRIs” document was prepared by Dr David Healy at the request of the MHRA, following their personal meeting in September 2008 with Seroxat campaigner Bob Fiddaman (SEROXAT SUFFERERS blog) who brought up the matter of an SSRI Withdrawal Protocol and suggested they liaise with the UK’s Leading Authority on the SSRI, SNRI drug class to facilitate its production. The document was presented to the MHRA in June 2009.
The David Healy document “Halting SSRIs” states -
"There are 2 theories about what leads to dependence and withdrawal that dictate slightly differing management plans.
One theory is that the relatively short half life of paroxetine and venlafaxine make these two drugs more problematic. This leads to a withdrawal strategy that advocates switching from paroxetine or other drugs to fluoxetine.
The second is that paroxetine and venlafaxine are relatively more potent serotonin reuptake inhibitors and this theory leads to a switch to less potent serotonin reuptake inhibitors such as citalopram.”The theories highlight two problems - the drugs shortness of half-life and the drugs potency as a serotonin re-uptake inhibitor.
A drugs half-life is the average period of time the drug takes to reduce to or by half its original concentration once ingested - i.e. from 50mg to 25 mg, then from 25mg to 12.5 mg etc.
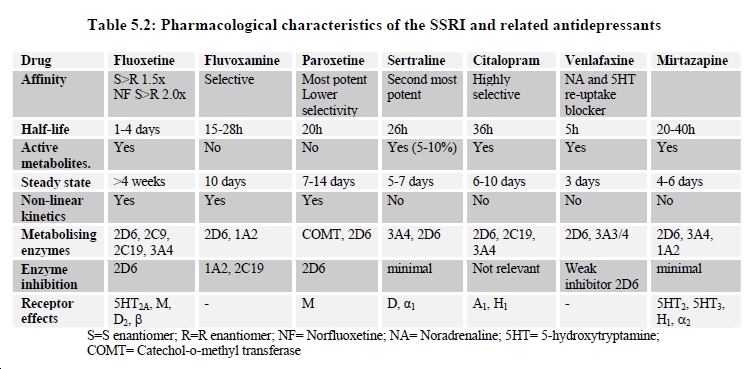
If the discontinuation problems are due to the short half-life of the drug - the December 2004 Committee on Safety of Medicines (CSM), Expert Working Group (EWG) on SSRI Antidepressants Report table 5.2 (below), shows that venlafaxine (Wyeth, Efexor UK, Effexor USA) has the shortest half-life at 5 hours, followed by paroxetine (GSK, Seroxat UK, Paxil USA) at 20 hours and sertraline (Pfizer, Lustral UK, Zoloft USA) at 26 hours.

{kind=link}
………NB – The CSM Report was carried out prior to the SNRI duloxetine (Eli Lilly, Yentreve, Cymbalta) being licensed.
The CSM, EWG report table 5.2 also indicates the drugs potency as serotonin re-uptake inhibitor and their affinity to monoamine transporters (MAT) – the selectivity of which has a bearing on the of the drugs classification.
Venlafaxine is classified by some as an SNRI, although in 1998 venlafaxine was listed in the Prescription Cost Analysis (PCA) statistics and British National Formulary, BNF: 4 . 3 . 3 . 0 SSRI section, in 1999 it was moved to PCA, BNF : 4 . 3 . 4 . 0 “Other Antidepressant Drugs” section where it remains. It’s unclear whether this was at Wyeth, the manufacturers, request or a licensing classification decision.
In the “HALTING SSRIs” document Dr David Healy explains the following –
““SSRI stands for selective Serotonin reuptake inhibitor. This does not mean these drugs are selective to the serotonin system or that they are in some sense pharmacologically “clean”. It means they have little effects on the norepinephrine/noradrenaline system.”In the same document he also explains the following –
“Venlafaxine in doses up to 150 mg is an SSRI. Over 150 mg it also inhibits noradrenaline reuptake. Duloxetine is a potent serotonin reuptake inhibitor but not selective to the serotonin system.”Venlafaxine is the only drug in the SSRI, SNRI class with a recognised additional mode of action that is dose specific -- > 150 mg Selective Serotonin RI – 150 mg > Serotonin Noradrenaline RI - 300 mg > Serotonin Noradrenaline Dopamine RI.
It would appear that if the Discontinuation Issue were solely dependant on the individual drugs half-life, venlafaxine with a 5 hour half-life would be considered the worst drug. However, the Seroxat Group Litigation Order No: 68 Defining Issue wording specifically states -
“than all other Selective Serotonin Re-uptake Inhibitors (SSRIs)”all drug in the class are classified Re-uptake Inhibitors (RI) - can the SNRI venlafaxine with it's recognised mode of Selective Serotonin RI action in doses up 150 mg be considered an SSRI? Are other SSRIs in the drug class, including Seroxat, which also have affinities to Noradrenaline and Dopamine correctly classified?
It's not only the discontinuation but the effects this drug Seroxat has on your emotions and how it effects your day to day life.This drug should never have been allowed to be prescribed GSK do not care about anything but money they are a inhumane company and should pay for the damage they have caused to people's lives.
ReplyDelete